
For years, distinguished pathologist Cyril Wecht, MD, JD has expressed doubts that Kennedy’s throat wound was an entry because no one could tell him where the bullet went. “The throat is all soft tissue, where did it exit?"
Good question, but it’s based on the premise that if the bullet had been found … we would know about it.
Well, we don’t know where that bullet went, but we do know about another bullet that was found—but never mentioned in the official record.
A Navy doctor published an obscure memoir in which he reports that petty officers sent to retrieve bone fragments from JFK’s car also found a misshapen, but whole bullet in the back of the car. (Official reports only mention bullet fragments, and they were found in the front of the car.)
That doctor, James Young, briefly inspected it, then gave it back to the petty officer who gave it to James Humes, the lead pathologist. Then where did it go? Humes made a big show of looking for bullets that night.
Young was puzzled when, years later, he could find no report on that bullet. He wrote to President Gerald Ford asking about it, and got a useless response. We have researcher Randy Robertson to thank for this discovery. (To see more on this, please go here.)
Maybe you can’t quite believe the above story, but you should be even more skeptical of anything you are told by the government. And you should wonder about what you are not told.
Humes et al Suppressed Fundamental Evidence:
(1) Kennedy’s cerebellum. You will not find one word about it in the main autopsy report, which only describes the upper brain, as well as organs not even relevant to the murder. Nor will you find mention of it any of Humes’s testimony. (The supplementary report mentions a microscopic analysis of a small piece of it.) The Parkland Hospital doctors described massive damage of this organ, damage inconsistent with the official narrative. (For more on this, go here and here.)
(2) Kennedy’s throat wound. Humes et al pretended they were completely unaware of it on the night of the autopsy, when the body was still available. And so they did not document it or explore it further. Years later, a pathologist who assisted Humes, said they saw the remains of the bullet hole itself, “part of the perimeter of a bullet wound in the anterior neck.” (For the complete story on this, go here.)
And so again I ask, why assume no bullet entered JFK’s throat because you don’t know where it went?
Throat Wound: Abrasion/Contusion Collar
Not long ago, I saw an email in which a researcher said Kennedy’s throat wound had no abrasion collar. He didn’t say that he saw no report of one, or that blood obscured the wound so that none was seen (a lone nutter claim). He just omnisciently asserted that none had existed. People are entitled to their opinions, but they should be given along with all the facts readers need for making up their own minds.
Here is probably the most relevant fact of all: When Malcolm Perry—the Parkland Hospital doctor who worked on the throat wound—was specifically asked by the HSCA to describe the wound’s edges, he included these words: “The edges were bruised.” A bruise is a contusion. Perry seems to have been referring to a contusion collar—which, like an abrasion collar, is definitive of an entrance wound.
Some authors use the expressions “abrasion” and “contusion” rings or collars interchangeably. But though related, they are not the same. Both are said to be caused by temporary over-stretching of the skin. And the skin on the perimeter of the bullet hole is abraded. A few millimeters away, damaged blood vessels in the dermis bleed beneath the skin, resulting in a visible bruise. Here’s an illustration from an article on the characteristics of entrance wounds by jacketed bullets, fired at a distance.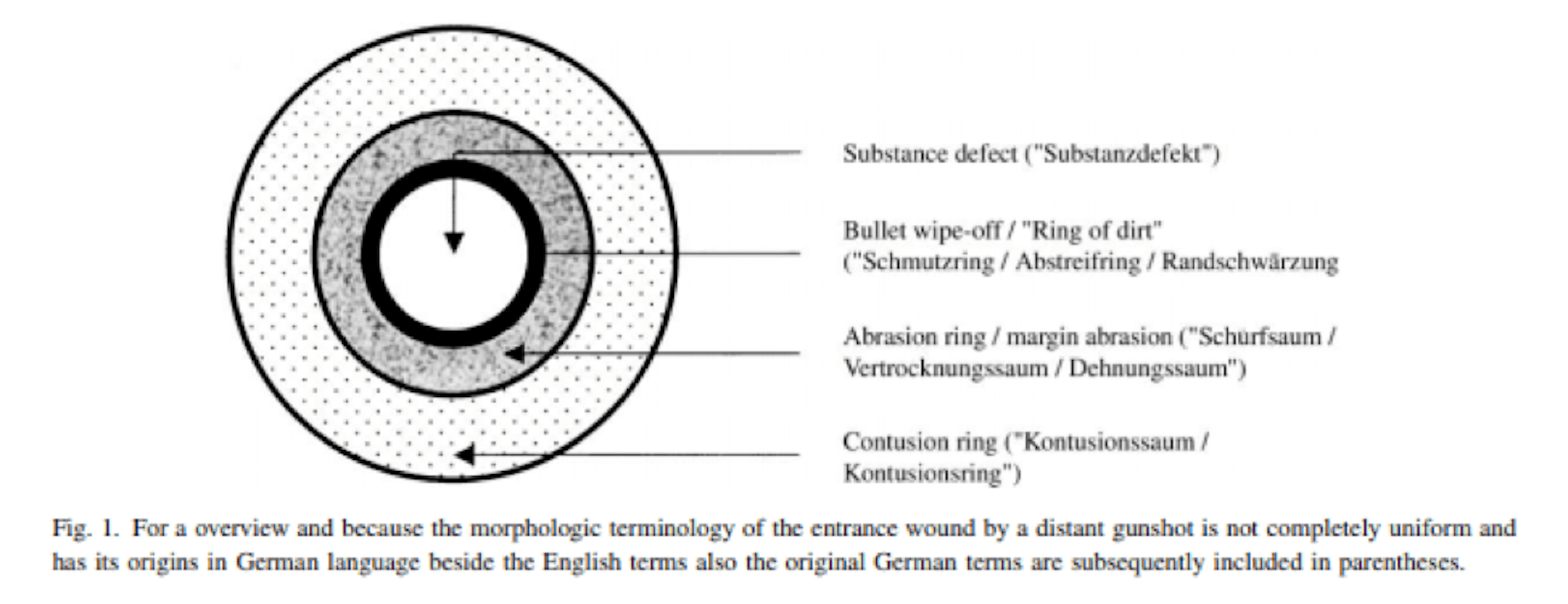
Note: Jacketed bullets from centre fire rifles do not always cause abrasion collars. Also, entrances can have slightly ragged edges. (Gunshot Wounds Aspects of Firearms, Ballistics, and Forensic Techniques, Second Edition, by Vincent J.M. Di Maio, MD, CRC Press, 1999.)
To the Warren Commission, Perry had described a typical entrance wound: “approximately 5 mm in diameter…exuding blood slowly which partially obscured it. Its edges were neither ragged nor punched out, but rather clean.”
Later he was again asked about the wound, and this time Commissioner Arlen Specter clarified something significant. Perry seems to have said the wound was “not punched out,” but he also said it was “not pushed out.” Specter specifically asked if the wound was “pushed out”—“everted” in the language of forensics—and characteristic of an exit. Perry said it was not. (Nor did he say it was pushed in.)
Don Thomas: Throat Wound Was an Exit
In his book Hear No Evil. Politics, Science & the Forensic Evidence in the Kennedy Association (Mary Ferrell Foundation Press, 2010), Donald Byron Thomas promotes the idea that the wound was an exit.
The author seems to believe the back and throat wounds were proven to be connected when in fact there was no proof. This was an inference based on incomplete information. Very few researchers claim the back wound was anything but an entrance, but we cannot explain where that bullet went. Since it created such an apparently shallow wound, it may have fallen out. It may have been the slightly bent bullet found in the limousine.
As for explaining what happened to the bullet that we say entered the throat, we cannot. But, based on all the other key evidence that went unreported, it’s not unreasonable to assume that if it had been found during the autopsy, it would not have been reported. (Thomas does not mention any of the known suppressed key evidence described above.)
Thomas also seems to believe the pathologists who performed the autopsy saw no evidence of the bullet wound in the throat. On page 238 of his book, he said “The precise nature of the wound cannot be determined because the wound was obliterated.” In fact, it was only bisected, not obliterated and, as mentioned above, one of the pathologists reported seeing part of it.
The author does not report any of the telling details Perry described, aside from the wound’s smallness. And instead of providing recent information on wounds, Thomas quoted from a not very informative book written in the early 1920s:
Provided no bone lesion is present, the exit aperture is often difficult to discriminate from the entrance wound. The two wounds maybe [sic] equal in size, the entrance wound may show inverted edges, while in the exit wound the edges are generally everted [pushed out]. When the bullet has passed through soft parts alone, the exit wound is apt to be circular in shape. (Thomas, p. 238) [Emphasis added.]
But Perry had specifically said the edges were not everted, that is, not pushed out. More important, Thomas said nothing about the bruised edges.
An Invalid Explanation for Wound’s Smallness
Thomas said that, though the wound was small, it was still an exit, and its size could be explained by the phenomenon of “shoring” or “buttressing.” Meaning the skin was held in place by Kennedy’s collar and necktie. And he quoted experts who say that when the skin is held in place by something, like a wall, floor, chair back, or supportive clothing, the bullet can’t stretch the skin outward until it tears (one reason why exits are small and star-shaped)—and a small “shored” wound is created.
But for this to be possible, the wound has to be right behind the shoring material.
Parkland Hospital’s Charles Carrico, MD—who saw the wound while Kennedy was still fully dressed—said the wound was “right above” the neck tie. And Malcolm Perry, the doctor who cut across the wound, said the bullet struck at the level of the second or third tracheal ring, just below the Adam’s apple.
Instead of deferring to these doctors who provided facts, Thomas gave his opinion, based on a photo showing JFK in an unnatural position with his neck hyperextended: “… it would seem more likely that the bullet passed below the necktie.” (p. 236)
Below the necktie? As you can see from this photo, his Adam’s apple is well above his collar and necktie.
Though Thomas disagreed with what Carrico said about the wound’s location, he argued the idea of shoring even if Carrico was right: The amount of buttressing would still be appreciable whether just above or just below the exiting bullet’s path.” (p. 236) He did not buttress this assertion with any references.
Here’s another good reason to doubt the wound was buttressed. Take a close look at what actually happens: Skin between the outgoing bullet and the buttressing material is crushed, and it becomes stuck to the material. When that material is pulled away, it creates a wide abrasion collar consisting of skin tags that resemble a peeling sunburn. More important—grossly visible skin is left behind on the material. (Am J Foren Med Path 1983; 4(3): 199-204)
The FBI closely inspected Kennedy’s shirt and tie, and did not report seeing skin on either garment.
Relevance of Bullet Velocity
What Malcolm Perry said about the internal damage in the neck reveals that if a bullet entered the throat, it was probably traveling at medium velocity (as defined circa 1963.).
There’s some concussive damage to surrounding organs—these are the kind of things one sees with gunshot wounds, in a blast injury ... And with high velocity, we do see a lot. Now the low velocity stuff, it’s often just a track, a wound track, with very little concussive or blast injury. This one was in between. There was evidence of some blast injury, but not like, say, what one sees with a high velocity rifle, like a 3006 or 223 ...
A bullet traveling that fast would have left a much larger exit wound. And this was proven by Army experiments involving the assassination of goats.
Yet other experiments proved that when non-deformed jacketed bullets exit straight out—as opposed to sideways—the size of the wound created is directly proportional to their exiting velocity. (J Trauma 1963; (March) 3(2): 120-128, p. 122) (Gunshot Wounds: Aspects of Firearms, Ballistics, and Forensic Techniques, Second Edition, by Vincent J.M. Di Maio, CRC Press, 1999.) (Thomas did not report this, but possibly he was unaware of these experiments.)
Translated: When all other things are equal, the slower the bullet, the smaller the exit wound. Put another way, the smaller the exit, the slower the bullet.
Translated further: If a bullet really did exit the president’s throat, it would not likely have had the energy to make it through Connally’s mohair jacket, let alone his chest and wrist.
And there goes the Single Bullet Theory.
